Since nearly a quarter of individuals aged 2-19 years are classified as obese in the United States, finding effective weight loss solutions to combat this epidemic are essential. Over time childhood obesity usually develops into adolescent and adult obesity contributing to increased prevalence of chronic disease and increased healthcare costs. The purpose of this review is to evaluate the physical and financial costs and benefits and of surgical versus lifestyle treatment interventions for adolescent obesity. Interventions include bariatric surgery and behavioral treatment incorporating components of family support, stimulus control, mindfulness when eating, self-monitoring, increasing physical activity, and managing daily intake. A theory based multicomponent behavioral intervention that includes the child and parent appears to be most successful for younger children. Nevertheless, often these children become obese adults, resulting in numerous treatment interventions. As adolescents become more independent these behavioral interventions are less successful long term. Bariatric surgery may be a life/cost saving alternative to treat obese adolescents. The main costs associated with surgery includes monetary expense of surgery, long-term vitamin/mineral deficiencies, and lifestyle adherence post-surgery.
Surgical complications are no higher in adolescents than adults, however, long term effects on growth remain to be seen. Overall, the age of onset of obesity influences the type of treatment individuals should participate in. Children with obesity younger than 10 years are more likely to respond to behavioral treatment than children with obesity older than 10 years. Adolescents with obesity who are 21 years and younger may respond better to a more aggressive approach of treatment, such as bariatric surgery. Analysis of child and adolescent lifestyle, environment, and support should be conducted to find a successful weight loss intervention.
Since nearly a quarter of individuals aged 2-19 years are classified as obese in the United States, finding effective weight loss solutions to combat this epidemic are essential. Over time childhood obesity usually develops into adolescent and adult obesity contributing to increased prevalence of chronic disease and increased healthcare costs. The purpose of this review is to evaluate the physical and financial costs and benefits and of surgical versus lifestyle treatment interventions for adolescent obesity. Interventions include bariatric surgery and behavioral treatment incorporating components of family support, stimulus control, mindfulness when eating, self-monitoring, increasing physical activity, and managing daily intake. A theory based multicomponent behavioral intervention that includes the child and parent appears to be most successful for younger children. Nevertheless, often these children become obese adults, resulting in numerous treatment interventions. As adolescents become more independent these behavioral interventions are less successful long term. Bariatric surgery may be a life/cost saving alternative to treat obese adolescents. The main costs associated with surgery includes monetary expense of surgery, long-term vitamin/mineral deficiencies, and lifestyle adherence post-surgery.
Surgical complications are no higher in adolescents than adults, however, long term effects on growth remain to be seen. Overall, the age of onset of obesity influences the type of treatment individuals should participate in. Children with obesity younger than 10 years are more likely to respond to behavioral treatment than children with obesity older than 10 years. Adolescents with obesity who are 21 years and younger may respond better to a more aggressive approach of treatment, such as bariatric surgery. Analysis of child and adolescent lifestyle, environment, and support should be conducted to find a successful weight loss intervention.
Over the past 20 years, the prevalence of childhood and adolescent obesity has reached epidemic proportions as nearly a quarter of children and adolescents aged 2-19 years are considered obese [1]. The good news is that the prevalence of obese children aged 2-5 years has decreased from 14% to 8% over the last few years [1]. Therefore, children aged 6-11 and adolescents aged 12-19 years constitute the bulk of the childhood obesity epidemic [1] and should be the focus of treatment options. Obesity status among children and adolescents aged 2-19 years of age is derived from Body Mass Index (BMI) and growth charts from the Center for Disease Control. Obesity is defined as BMI at or above the gender-specific 95th percentile [2].
Not all children are at equal risk of developing childhood obesity. For example, childhood obesity rates in the United States differed among the education level of head of household and child’s ethnicity [3]. Obesity rates for children who live in an environment where the head of household finished college are nearly half that of children whose head of household did not complete high school. Non-Hispanic white children who live in an environment where the head of household completed college had the lowest prevalence of obesity. This was not the case for non-Hispanic African American boys, who showed no significant relationship between obesity and the level of education of the head of household [3]. There are several explanations for this difference in obesity rate, some of which may be attributed to the schools the children attended, peer pressure or whether the individuals were strength training [4].
Although evidence is mixed regarding the association between ethnicity and obesity, research suggests a strong relationship between preschool aged children obesity rates and low-income families, which may be associated with the head of household’s education level. Childhood obesity prevalence was highest in preschool aged children 2-4 years from families with less than a 100% poverty income ratio (PIR) [5].
Over time, childhood obesity usually develops into adolescent and adult obesity, contributing to increased prevalence of obesity, diabetes, hypertension, hyperlipidemia, and overall healthcare costs for future generations [6]. Childhood obesity not only places the child’s physical health at risk, it also diminishes the mental health status of children and adolescents because psychosocial functioning decreases with increased BMI [4]. Today’s youth are endangering their future physical and mental capabilities as well as their financial stability; therefore, this epidemic needs to be stopped. Moreover, there is a need to assess the most safe, cost effective way for adolescents to lose weight and keep it off.
What is best way to stop this adolescent obesity epidemic from spreading? Perhaps the best way to determine that is by completing a cost-benefit analysis of various treatment options for adolescent obesity which compares the total expected cost against the total expected benefits of each treatment option. In retrospect, the treatment option benefits should overshadow its costs in the long-term.
There are two main interventions to treat adolescent obesity; behavioral treatment and surgical weight loss procedure [4, 7]. Recommendations are constantly changing and much conflict revolves around these two distinct treatment options [8-10]; however, by using cost-benefit analysis, a systematic approach may be used to determine which treatment option is best for obese individuals in the long-term. The purpose of this review is to evaluate the physical and financial costs and benefits of surgical versus behavioral treatment interventions for adolescent obesity.
This study is a literature review of articles related to adolescent weight loss: lifestyle methods or bariatric surgery. Pubmed, Web of Science, and GoogleScholar databases were searched using the key words adolescent, bariatric surgery, weight loss surgery, cost benefit analysis of adolescent bariatric surgery, prevalence of adolescent obesity, lifestyle interventions for adolescent obesity, and surgical solutions for adolescent obesity. The references in these articles were reviewed for additional articles. Articles for this review included original research, literature review articles, quantitative, and qualitative studies in the English language. The selected articles in this review focused on bariatric surgery or lifestyle interventions as a solution for the rising adolescent obesity rates and the cost-benefit relationship between lifestyle interventions and bariatric surgery.
Out of 212 articles found, 28 articles were chosen for inclusion in this literature review. Through these articles, a cost-benefit relationship was examined between adolescent obesity and adolescent bariatric surgery.
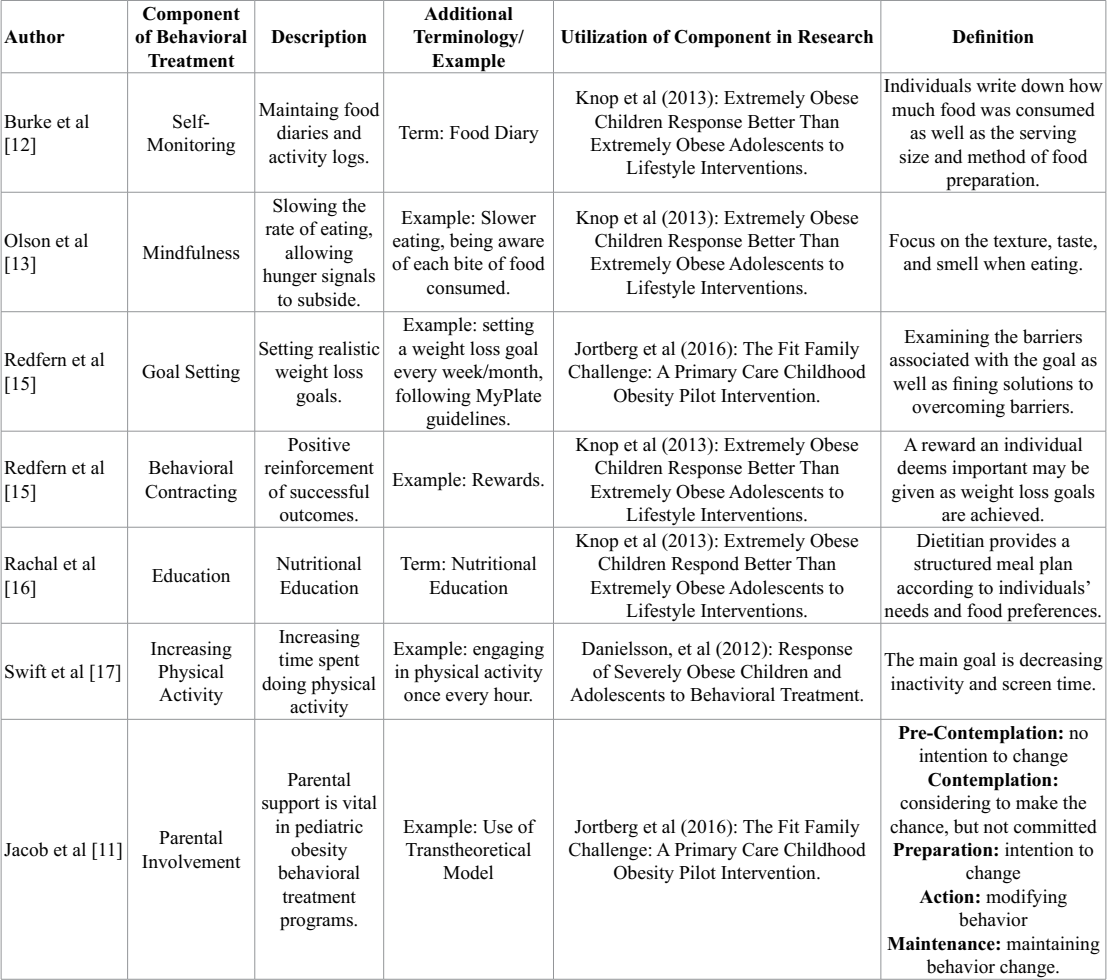
Table 1: Types of Behavioral Treatment Components.
Behavioral Therapy
Often considered the first line of treatment for obesity, behavioral based therapy involves a structured diet and exercise regime plus other behavioral based components. Much like adult weight loss programs, pediatric weight loss programs incorporate various aspects of behavioral therapy. However, unlike adult weight loss programs, parent involvement and parent modeling of healthy behaviors are essential in pediatric weight loss programs as the most successful weight management programs are family based [4].
Behavioral therapy encompasses a variety of methods including self-monitoring, stimulus control, slower eating, goal setting, behavioral contracting, education, increasing physical activity, and parental involvement [11]. See Table 1. Self-monitoring through food diaries and/or activity logs, allows individuals to track daily activities [12]. Stimulus control allows environmental modification to prevent overeating. For instance, limiting the availability of non-nutrient dense food items in an individual’s home creates an encouraging environment to eat healthfully. Eating at a slower rate embodies mindfulness, allowing individuals to focus on food texture, smell, and taste [13, 14]. Behavioral contracting and goal setting go hand in hand as positive reinforcement (i.e. rewards) aid individuals in meeting their weight loss goal [15]. Nutrition education provides skill development to create a structured meal plan per one’s needs and food preferences. This is key for both children/adolescents and parents [16]. Increasing physical activity assists in positive reinforcement because it decreases screen time and increases fat loss [17]. Finally, social support and parent involvement are of upmost importance in pediatric behavioral therapy because both hold the power to instigate behavior change [11, 14]. Table 2 provides research studies that showed benefits of using behavioral treatment methods (Tables 1,2).
Furthermore, incorporation of a family-focused behavioral modification program into primary care practices for children aged 6-12 years dramatically improved BMI and lifestyle factors associated with obesity. These lifestyle factors included daily fruit and vegetable intake, physical activity, screen time, number of times spent with family activity, intake of sugar-sweetened beverages, and number of times eating out each week [18]. Moreover, when incorporating family into a behavioral therapy lifestyle intervention, a parent’s readiness to change should be evaluated using the Transtheoretical Model [11]. Defining a parents’ readiness for change allows for a more individualized plan of care, leading to child adherence of behavioral therapy.
Furthermore, incorporation of a family-focused behavioral modification program into primary care practices for children aged 6-12 years dramatically improved BMI and lifestyle factors associated with obesity. These lifestyle factors included daily fruit and vegetable intake, physical activity, screen time, number of times spent with family activity, intake of sugar-sweetened beverages, and number of times eating out each week [18]. Moreover, when incorporating family into a behavioral therapy lifestyle intervention, a parent’s readiness to change should be evaluated using the Transtheoretical Model [11]. Defining a parents’ readiness for change allows for a more individualized plan of care, leading to child adherence of behavioral therapy.
The Transtheoretical Model may also be used to measure a child’s or adolescent’s readiness to change in regards to living a healthful lifestyle that facilitates weight loss. Children and adolescent readiness to change is largely influenced by their age. Younger children (< 10 years) are more likely to be under the control of parents; while older adolescents (> 10 years) are less likely to be influenced by their parents. As children grow into adolescents they also experience more peer pressure, which may dictate what they eat or the activities in which they participate [8, 11, 19]. In multiple behavioral therapy intervention studies, children between the ages of 6-10 years showed a greater decrease in BMI compared to adolescents aged 10-16 years [8, 11, 19]. These results show lifestyle intervention to be effective for extremely obese children, but not necessarily for extremely obese adolescents.
Cost of Behavioral Therapy
Although behavioral therapy is considered the first line of treatment for adolescents with obesity, yet many researchers and health professionals are unaware of its long-term effectiveness. This lack of evidence concluding behavioral therapy works in the long-term leads to assumptions of failed attempts at weight loss. Thus, behavioral therapy for adolescent weight loss may not be effective in the long run. Individuals, especially adolescents, may not adhere to behavioral therapy due to decreased motivation, increased preference for non-nutrient dense foods, increased hunger, lack of physical activity, and time constraints [20]. These costs may be due to peer pressure, lack of patience, and basic growth needs of adolescents. Peer pressure may cause obese adolescents to engage in the same activities as friends. Rather than participating in sports, they may go to a friend’s house and play video games.
Additionally, individuals’ motivation may decrease as time goes on without any weight loss. Adolescents are generally impatient, and they need the help of their support systems to keep them motivated to lose weight [9,18-19]. Moreover, adolescents may just be naturally hungry because they are growing and need enough nutrients to grow to a healthy weight [4]. This may dampen weight loss efforts. Obesity treatment options for the adolescent age group may need to rely on more extreme options, such as surgery.
Bariatric Surgery Treatment
An alternative treatment to behavioral therapy is bariatric surgery for obese adolescents; however, this option is only considered after behavioral therapy has failed. It is argued that bariatric surgery is an effective method to alleviate obesity in adolescents compared with behavioral therapy techniques. Adolescent bariatric surgery has increased in popularity as there were approximately 1600 surgeries completed per year since 2009, with the three most common surgeries including Laparoscopic Adjustable Band (LAGB), vertical sleeve gastrectomy (VSG), and Roux-en-Y-Gastric Bypass (RYGB) [7]. Table 3 shows the types of bariatric surgery with benefits and complications of each type of surgery.
Laparoscopic Adjustable Gastric Banding
Laparoscopic adjustable gastric banding (LAGB) involves insertion of an inflatable silicone elastic band dividing the stomach into an upper and lower section connected by a channel, causing food to empty into the lower section at a slower rate. LABG has a quicker recovery time and shorter hospital stay; however, long-term weight loss is likely less [21-24].
Vertical Sleeve Gastrectomy
The vertical sleeve gastrectomy (VSG) reconstructs the stomach and takes place by stapling along the greater curvature of the stomach in order to decrease stomach size, but maintain digestive/gastric emptying processes [9]. The VSG results in fewer nutrient deficiencies, reduced appetite, and early satiety along with remission of diabetes mellitus; however, VSG sleeve leakage may occur over time [25]. Moreover, excess weight loss is greater than LAGB and similar to LAGB, this surgery results in decreased nutrient defiencies [26]. However, the hospital stay for VSG is longer than with LAGB [9, 26].
Roux-en-Y Gastric Bypass
Finally, Roux-en-Y-Gastric Bypass (RYGB) divides the stomach into two sections, with the upper part being a small pouch that connects to the jejunum using a Y-shaped limb of small intestine; causing food to bypass the duodenum. Digestive secretions mix chyme at the junction of the jejunum and duodenum. RYGB has a high successful rate for weight loss and reduction of obesity-related comorbidities, such as diabetes, hypertension, and hyperlipidemia; however, it also can cause severe nutrient deficiencies, including vitamins B-12 and D, iron, copper, calcium, and even protein [26, 27].
Adolescent Bariatric Surgery Eligibility.
Similar to adults, adolescents may be eligible for bariatric surgery if they have a BMI ≥ 35 kg/m2 with a severe comorbidity; comorbidities may include moderate to severe obstructive sleep apnea, type ll diabetes, hypertension, or nonalcoholic steatohepatitis. Adolescents may also be qualified for bariatric surgery if they have a BMI ≥ 40 kg/m2 with a less severe comorbidity. Exclusions to surgery include those with substance abuse as well as psychosocial, medical, or cognitive conditions. These conditions often prevent adherence to recommendations and the inability to understand the risks and benefits of weight loss surgery. The main long-term complications associated with bariatric surgery in children and adolescents include nutrient deficiencies, especially vitamin B12, thiamin, vitamin D [7] and even protein associated with low calorie intake after surgery [27]. However, often times the benefits, such as remission of diabetes, hyperlipidemia, hypertensions, and sleep apnea outweigh the monetary and physical costs of surgery [7].
Adolescent Bariatric Surgery
Research has been conducted to evaluate the success and safety of bariatric surgery and the effect surgery has on children and adolescent growth [7, 9, 28]. While short-term complications were lower in children and adolescents who underwent LAGB, BMI reductions were greater for children and adolescent who underwent RYGB [28]. Additionally, weight loss outcomes were the same for individuals younger and older than 18 years of age; thus, bariatric surgery in children and adolescents have the same short-term complication rates and weight loss results as adult surgeries [28].
As seen in Table 4, all bariatric surgical procedures approved for adolescents resulted in excess weight loss three years post-surgery [7, 9]. Excess weight loss after both RYGB and VSG in patients 21 years or younger were improved in comparison with weight loss in patients 22-59 years of age 3 years post-surgery. Therefore, both VSG and RYGB offer long-term weight loss benefits in individuals 21 years of age or younger [9]. Furthermore, RYGB, specifically, improved adolescent lipid levels, hemoglobin A1c, and obesity related symptoms in patients 1-year post-surgery [9].
Costs of Bariatric Surgery
Morbidly obese adolescents experience long-term weight loss using bariatric surgery. Adolescents found long-term success with weight loss, financial stability, and improved quality of life following bariatric surgery [29, 30]. Three years after surgery, individuals experienced an increase of 0.199 quality adjusted life years compared to adolescents who did not undergo bariatric surgery [29]. Bariatric surgery was not found to be cost-effective at three years post-surgery; however, became cost-effective five years post-surgery. Researchers suggest that adolescents who undergo bariatric surgery will save $157 per year, approximately [30]. With an improved quality of life, remission of comorbid diseases, and financial security, adolescent bariatric surgery supports individuals’ health status in the long-term.
Ardith Brunt, North Dakota State University, Department of Health, Nutrition and Exercise Sciences, Box 6050, Fargo, North Dakota 58108, USA.

 This work is licensed under a Creative Commons Attribution 4.0 International License © 2018 sciaeon.org
This work is licensed under a Creative Commons Attribution 4.0 International License © 2018 sciaeon.org